
A Patient’s Guide to Ulnar Nerve Entrapment at the Wrist
(Guyon’s Canal Syndrome)
Introduction
The ulnar nerve is often called the funny bone at the elbow. However, there is little funny about injury to the nerve. When this nerve is irritated either by trauma or compression—it causes pain, numbness, tingling or burning into the small finger and part of the ring finger.
The ulnar nerve is one of three nerves which make the hand work and feel. The ulnar nerve is responsible for approximately 50% of our hand strength. The most common site of compression of the nerve is the inside portion of the elbow—the cubital tunnel.
Ulnar nerve compression at the wrist is less common than at the elbow. Compression at the wrist (Guyon’s canal) is usually associated with repetitive trauma or ganglions.
Anatomy
The ulnar nerve, like all other peripheral nerves begins in the spinal cord and accesses the arm via the brachial plexus. As the nerve then travels down the arm, the nerve gains access to the arm at the level of the elbow on the inside (medial) aspect. The nerve travels through a defined space in the elbow termed the cubital tunnel. This “tunnel” which the nerve traverses is fixed in size—any inflammation of the tunnel causes compression of the nerve leading to numbness and tingling felt in the hand.
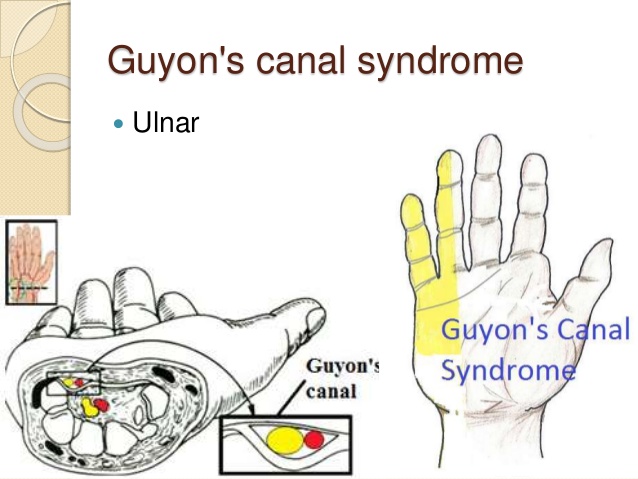
A right hand viewed in cross section showing the ulnar nerve and artery traversing Guyon’s canal.
There are three nerves which make a normal hand function. The radial nerve gives sensation to the top of the hand. The median nerve gives sensation to the thumb, index, middle, and the half of the ring finger on the thumb side. Classically, the ulnar nerve gives sensation to the small finger and part of the ring finger. The ulnar nerve also supplies most of the muscles of the hand and gives approximately 50% of the grip power for the hand. The ulnar nerve function allows the hand to work in smooth unison. This is the classic distribution and wide variation is known to exist.
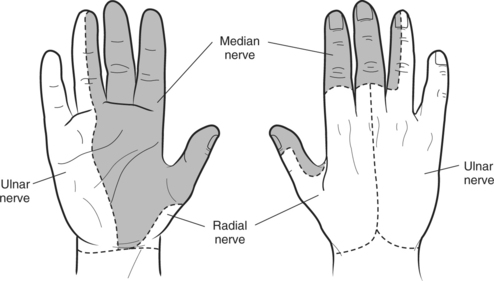
Classic innervation of the median nerve shown in grey for the right hand from the bottom and top. Note the distribution for both the ulnar nerve and radial nerve along the small/ring finger and top of hand.
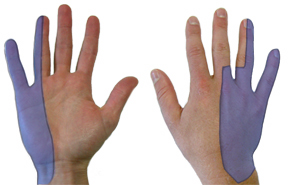
Classic innervation for the ulnar nerve shown in blue
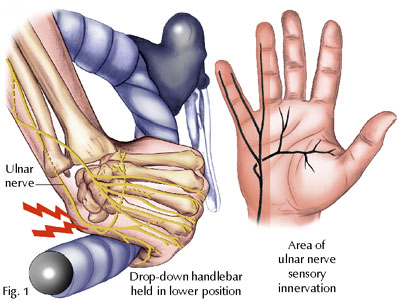
Repetitive trauma may be associated with the development of Guyon’s canal syndrome
Diagnosis
Symptoms
Patients report numbness, tingling or burning in the ulnar nerve distribution of the hand discussed above—small and part of ring fingers. The symptoms may be worse at night, as we tend to sleep without elbow flexed, further compressing the nerve. Patients may also notice the symptoms are worse during the day when the elbow is flexed with activity.
Hand Surgeon Examination
After determining your symptoms and detailing a history of your difficulties, a physical examination will be performed. Your hand surgeon will note the range of motion of your extremity. Further notice will be focused on the function of the nerves in the extremity.
Nerves give both sensation and muscular strength. How well the nerve functions may be assessed by your ability to determine sharp versus dull or the differentiation of two points. General examination of the hand may detail any muscular atrophy from severe nerve dysfunction. Your surgeon may also test muscular strength and note them for particular nerve function
Special testing for carpal tunnel includes tapping on the nerve at Guyon’s tunnel eliciting tingling (called a positive Tinnel sign). Other provocative tests for cubital tunnel (to differentiate compression at the elbow from Guyon’s canal) include pressing on the nerve at the tunnel or flexing the elbow (positive elbow flexion exam). Importantly, the surgeon may look for negative signs including neck compression (Spurling exam) or thoracic outlet or pronator syndrome.
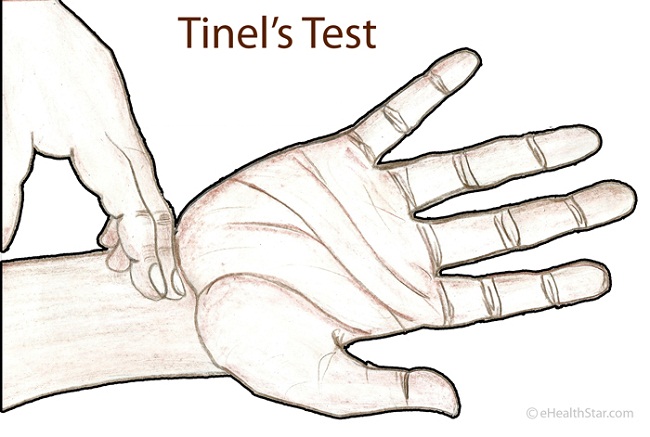
Tapping on the ulnar nerve at Guyon’s canal reproduces symptoms of tingling in the small and ring finger.
Testing
Electrophysiological tests evaluate the ability of the nerve to conduct electrical signals and the ability of muscles to respond to these signals. It should be noted that as in all tests, both false positives and false negatives are present. Therefore these tests are ordered to confirm the presence of carpal tunnel. However, these tests by themselves neither diagnose nor rule out carpal tunnel syndrome. These tests may be conducted by your hand surgeon or these tests may be performed by a neurologist.
Since x-rays routinely have not been found to be helpful in the condition, unless other entities are suspected they typically are not ordered for this condition.
Treatment
Nonsurgical Treatment
Non-surgical treatment is typically indicated early in the disease or if the symptoms are mild. Nonoperative treatment is typically more effective in these situations. Activity modifications may be helpful if the patient has vibratory exposure or repetitive hand gripping or trauma. Bracing may be utilized by your surgeon and is typically utilized at night for most patients. If symptoms are controlled by these measures, no further treatment is indicated.
Surgical Treatment
If the patient’s symptoms persist, despite nonoperative management, surgical treatment is the next logical step—called a Guyon’s canal tunnel release. All surgical management is centered on decreasing pressure on the ulnar nerve at the tunnel. Surgical treatment can be performed as an outpatient surgery, typically using regional anesthesia. A small incision is made on the inside portion of the wrist and hand –and the roof of the cubital tunnel is released—relieving pressure on the nerve.

An incision for treatment of Guyon’s canal syndrome
Rehabilitation
After surgery, a light wrap will be applied to your arm. In most cases, a dressing change is used and band aids are used to keep the incision clean and dry. The patient may begin using the fingers and thumb after surgery for light activity and increase activity as tolerated. Sutures are removed in about 2 weeks and continuation of grip strengthening is emphasized.
Improvement in sensation may occur faster in Guyon’s canal release than in cubital tunnel syndrome However, Night time sleeping is typically the first symptom to improve. Improvement of feeling in the digits moves from the site of incision and marches distally over time. The rate of improvement and overall recovery are inversely related to the severity of nerve pinch and its duration. Pain and discomfort decrease over time after surgery. Improvements in sensation and strength may continue up to 18 months after cubital tunnel surgery for severe cases. Hand therapy is typically not required after cubital tunnel surgery.
Standard surgical risks for surgery are applicable including infection, bleeding, and anesthetic risks. Most cases do not require prophylaxis for deep vein thrombosis.
Surgery for cubital tunnel yields good results in most cases. Results of treatment may be compromised by longstanding nerve compression or other nerve disease. Recurrence after treatment is uncommon, but may respond to additional treatment.

